
Series Introduction
This is the first article in a three-part series about hearing loss. Part 2 covers treatment options, and Part 3 will explore the experience of using hearing aids. Based on feedback, we will continue to publish more articles on this topic, providing deeper insights and actionable guidance for anyone who suffers from hearing loss, loves music, or wants to protect their hearing.
If there’s one thing we all agree on at Tech&Audio, it’s that music improves our quality of life.
For years, music has offered relaxation, comfort during painful times, a way to celebrate joy and mark special events. It accompanies many of us during workouts, daily tasks, and even through shifting moods.
Music is so deeply woven into our lives that it can even help communicate with people experiencing cognitive decline or conditions like Alzheimer’s disease.
How We Hear
The organ responsible for receiving sound is the ear, which consists of three main parts:
- Outer ear: The auricle (the visible part) collects sound waves and directs them into the ear canal, where they are amplified before reaching the eardrum, which vibrates with incoming sound.
- Middle ear: Eardrum vibrations move three tiny bones (ossicles), further amplifying sound.
- Inner ear: The cochlea, a fluid-filled, snail-shaped organ, converts vibrations into electrical signals. About 25,000 nerve endings are activated as the fluid moves, sending impulses through the eighth cranial nerve (auditory nerve) to the brain.
The brain is ultimately responsible for interpreting these signals, shaping each person’s subjective hearing experience.

Hearing Loss
Hearing loss can occur for many reasons throughout life, including genetics, infections, ear diseases, meningitis, ear or head trauma, loud noise exposure, earwax buildup, medications affecting hearing, and age-related decline.
Untreated hearing loss can affect not only hearing but also communication, speech, and cognition.
Age-Related Hearing Loss
Gradual hearing loss, called presbycusis, occurs with aging. In the U.S., more than half of adults over 75 experience some age-related hearing loss.
Three main types exist:
- Conductive – affecting the outer or middle ear
- Sensorineural – affecting the inner ear
- Mixed – combining both
Conductive hearing loss may be improved, while sensorineural loss is typically permanent and requires rehabilitation.
Common symptoms include difficulty understanding speech in noisy environments, asking others to repeat themselves, turning up the volume, or experiencing tinnitus (ringing in the ears).
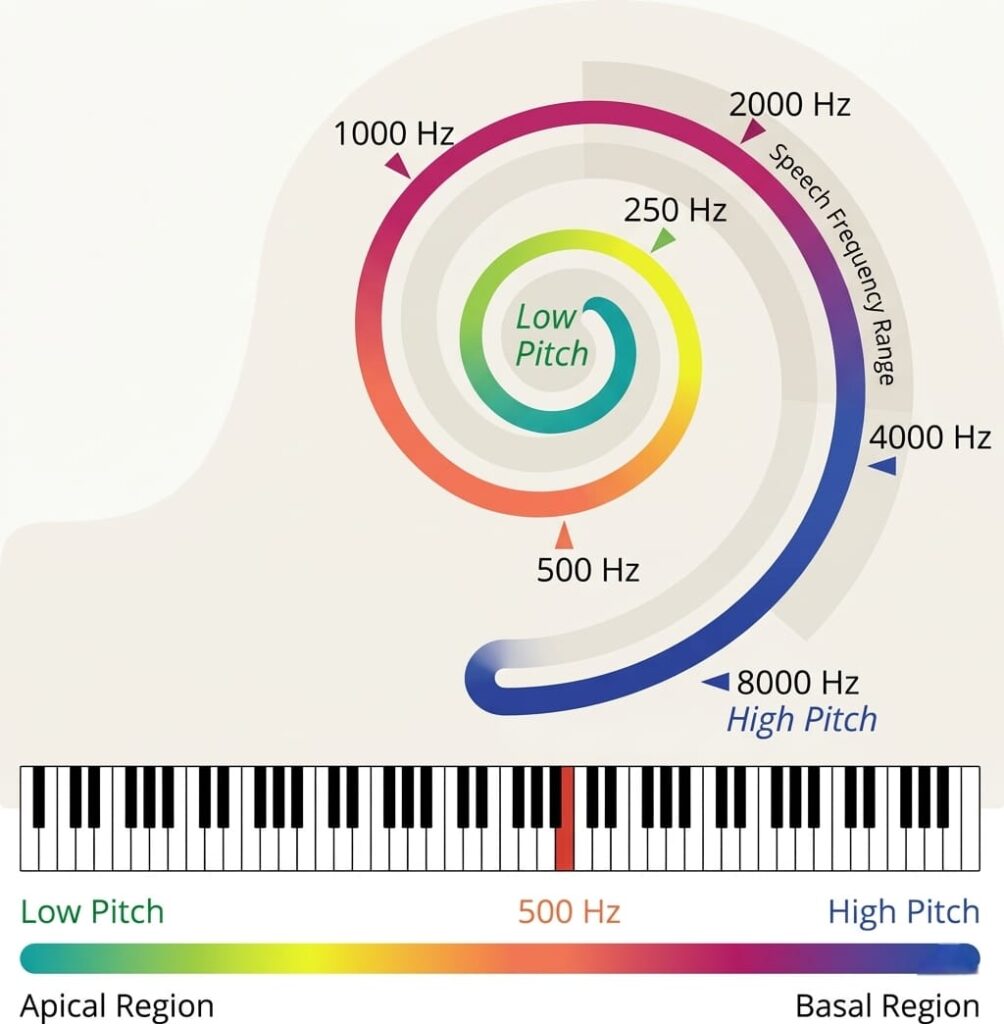
Understanding cochlear anatomy helps explain age-related hearing loss:
Hearing Test
I scheduled an appointment with an ENT (ear, nose, and throat) physician. My outer ear was clear, and I was referred for a professional hearing test. Hearing tests are available in hospitals and private clinics. Private clinics are often faster, avoiding long public system wait times.
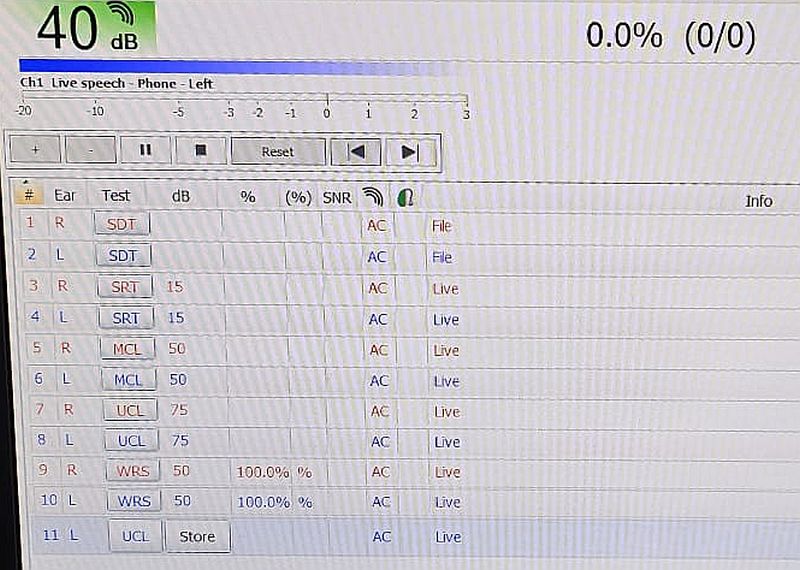
At the certified audiologist I conducted my test in a soundproof room using an audiometer. Each ear was tested separately in several stages:
- Speech Reception Threshold (SRT) – Repeat two-syllable words at decreasing volumes; threshold = lowest volume where ≥50% were repeated correctly.
- Speech Discrimination Test – Repeat single-syllable words; score = correct responses.
- Air Conduction – Threshold for pure tones 250–8000 Hz via headphones.
- Bone Conduction – Small device on mastoid bone tests inner ear directly; right ear = red triangle, left ear = blue triangle.
There are 2 stages of each cycle:
- First stage: words at ~15 dB, repeated.
- Second stage: shorter words. I indicated comfortable and too-loud volumes.
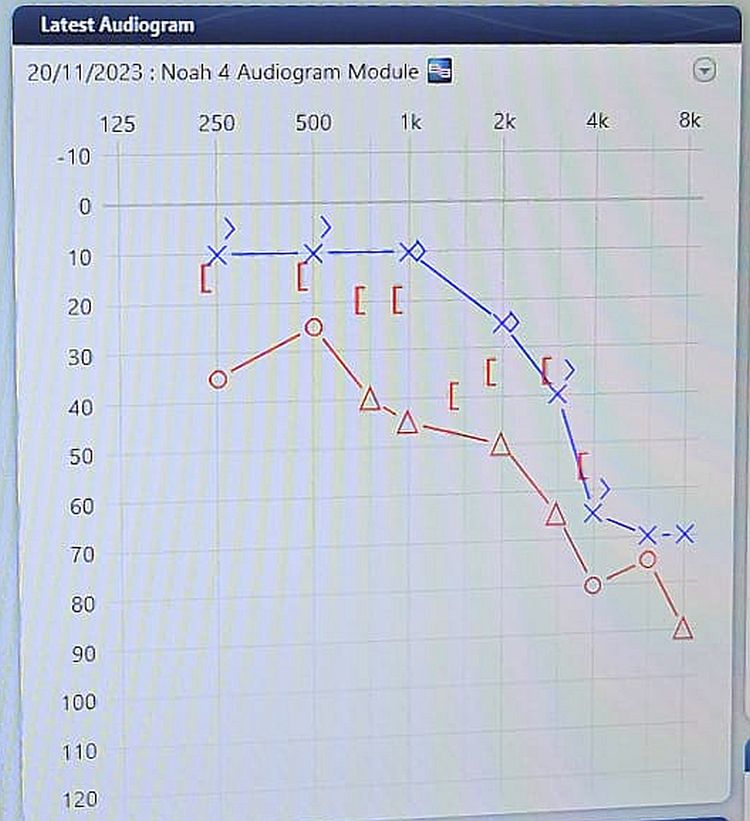
Next, ascending and descending tones (250–8000 Hz) measured the softest audible levels at each frequency, forming the audiogram.
Audiogram details:
- Right ear = red circles
- Left ear = blue Xs
- Horizontal axis = frequency (Hz)
- Vertical axis = intensity (dB)
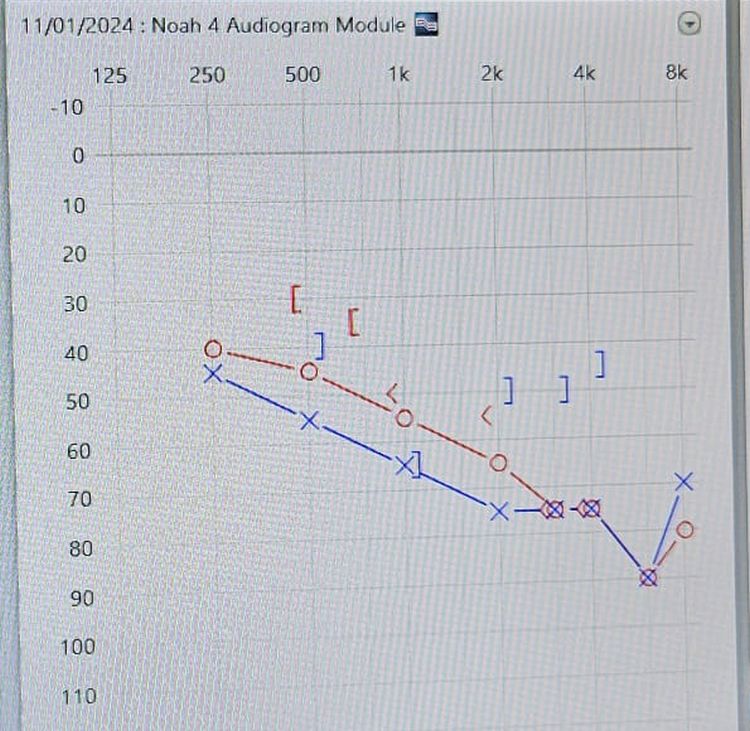
For perforated eardrums, hearing is tested directly in the inner ear. If inner-ear results are better than air-conduction, a conductive issue is suspected. The symbol “]” in the audiogram shows inner-ear results; the gap signals potential conduction problems.
Final step: eardrum pressure measured to confirm no fluid affected the results.
Treatment
Treatment for age-related hearing loss depends on severity. In most countries, hearing only above 40 dB is classified as moderate loss.
In the next article, we will explore how hearing aids work, cutting-edge technological developments, the role of high-tech industry, AI, and their added value for music lovers with age-related hearing loss.